
Rotator Cuff Tear & Repair
The rotator cuff is a group of four tendons that stabilise and power the shoulder joint. A tear in one or more of these tendons is one of the most common causes of shoulder pain in adults, and can result from a specific injury or gradual wear over time. Dr. Matthew Boyle is a fellowship-trained shoulder surgeon, and rotator cuff repair is one of the procedures he performs most frequently, drawing on extensive experience in both the diagnosis and arthroscopic repair of rotator cuff tears.
What is a Rotator Cuff Tear?
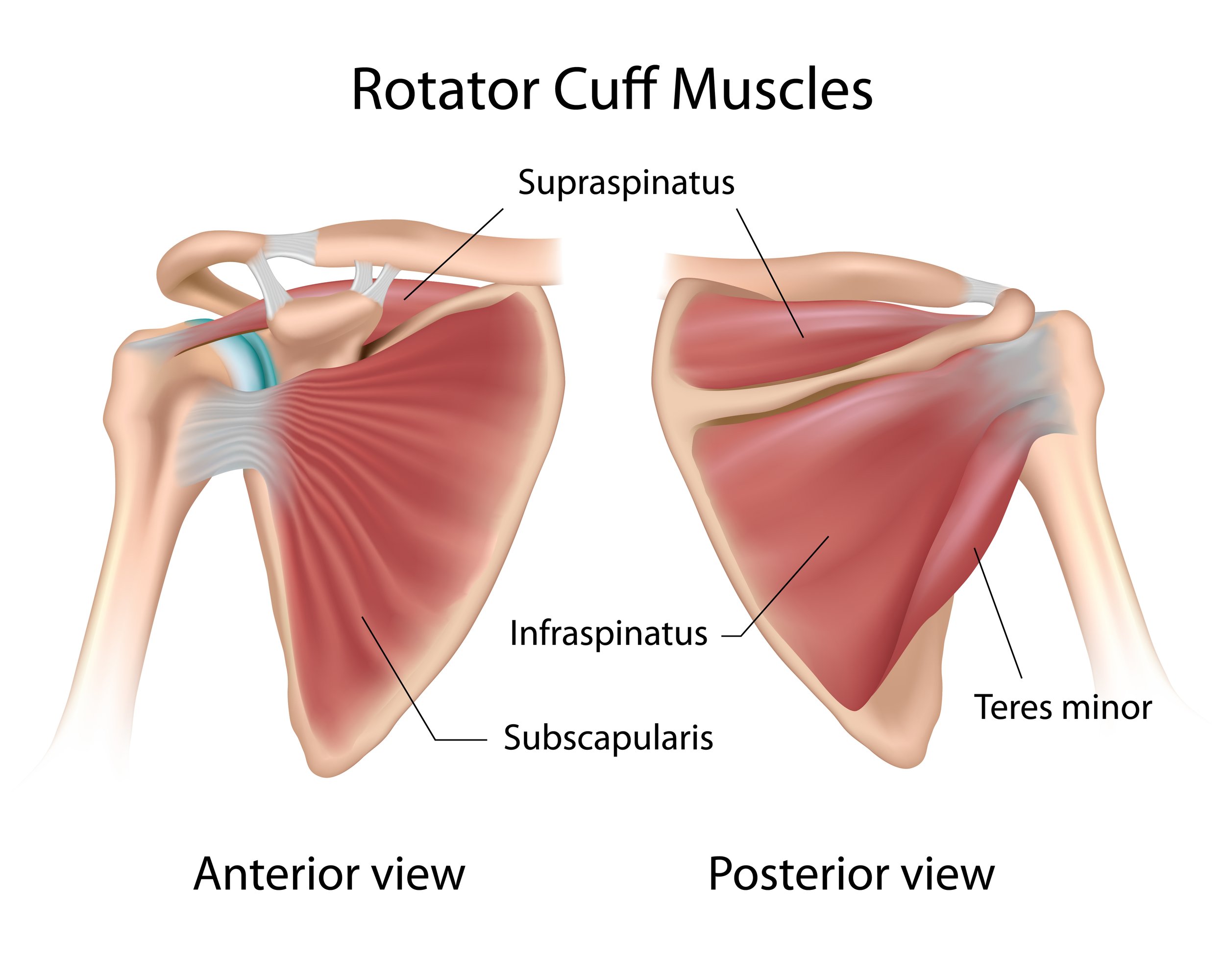
The rotator cuff is made up of four tendons - the supraspinatus, infraspinatus, subscapularis, and teres minor - that attach the scapula (shoulder blade) to the head of the humerus (the ball of the shoulder joint). These tendons work together to stabilise the shoulder and control its movement. A tear occurs when one or more of these tendons is partially or fully detached from the humerus bone, either through a specific traumatic event (e.g. a fall, a heavy lift, a rugby tackle) or through gradual tendon degeneration, which becomes more common with age.
Tears are generally classified as partial-thickness (the tendon is damaged but not completely detached) or full-thickness (the tendon has completely pulled away from the bone). The supraspinatus is the most commonly affected tendon.
Causes and Risk Factors
Rotator cuff tears fall into two broad categories:
Traumatic tears - caused by a specific incident, such as a fall onto an outstretched arm, a heavy or sudden lifting injury, or a sporting collision. These are more common in younger, active patients and are frequently seen after rugby, netball, and gym-related injuries in New Zealand.
Degenerative tears - develop gradually over time as the tendon weakens with age and repetitive use, often without a single triggering event. These are more common in patients over 50.
Risk factors for rotator cuff tears include age, repetitive overhead activity (tradespeople, throwing athletes), smoking (which impairs tendon healing), and a family history of rotator cuff problems.
Symptoms
Common symptoms of a rotator cuff tear include:
Pain with overhead movement or reaching behind the back
Weakness when lifting or rotating the arm
Night pain, particularly when lying on the affected shoulder
A catching, clicking, or grinding sensation with movement
In complete tears, a noticeable loss of strength or an inability to lift the arm normally
Symptoms can develop suddenly after an injury, or build gradually over weeks to months in degenerative cases.
Diagnosis
Diagnosis begins with a clinical examination, assessing shoulder strength, range of motion, and specific tests that isolate each rotator cuff tendon. Imaging is used to confirm the diagnosis and plan treatment:
X-ray - rules out fractures and assesses the bony anatomy of the shoulder, though it cannot directly show the tendons
MRI - the primary imaging tool for assessing tear size, location, tendon quality, and the degree of retraction, all of which influence treatment planning
Ultrasound - sometimes used as a quicker, lower-cost alternative for initial assessment
Treatment Options
Non-surgical management is appropriate for many partial tears and for some full-thickness tears in lower-demand patients, particularly older patients with degenerative tears and preserved function. This typically includes physiotherapy focused on rotator cuff and periscapular muscle strengthening, activity modification, and occasionally a corticosteroid injection for pain relief. Non-surgical treatment does not repair the tendon - the goal is to restore function and reduce pain using the remaining intact structures.
Surgical repair is generally recommended for:
Full-thickness tears in active or younger patients
Tears causing significant weakness or functional limitation
Tears that have failed an adequate trial of physiotherapy
Acute traumatic tears, where early repair typically gives better outcomes than delayed repair
Surgery is performed arthroscopically (through small incisions using a camera and specialised instruments) in the vast majority of cases. The torn tendon is reattached to the bone using small suture anchors, restoring the tendon's attachment and allowing it to heal back into position.
Recovery After Rotator Cuff Repair
Recovery from rotator cuff repair is gradual and follows a staged rehabilitation protocol:
0-6 weeks: Sling worn for protection; passive range of motion exercises only, no active lifting
6-12 weeks: Gradual introduction of active range of motion as the tendon heals
3-6 months: Progressive strengthening as healing allows
6-12 months: Return to full activity, including sport and overhead work, depending on the size of the tear and the demands of the activity
Rehabilitation timelines vary significantly based on tear size, tissue quality, and the specific repair performed - Dr. Boyle will provide a protocol specific to your procedure.
As one of the shoulder procedures Dr. Boyle performs most regularly, rotator cuff repair benefits from a well-established, refined surgical approach and a rehabilitation protocol that has been developed and adjusted over years of clinical practice.
Frequently Asked Questions
-
No - once a tendon has torn away from the bone, it will not reattach or heal on its own. Non-surgical treatment can improve pain and function using the shoulder's remaining structures, but it does not repair the tear itself.
-
For acute traumatic tears in active patients, earlier surgery generally leads to better outcomes, as delayed repair can allow the tendon to retract and the muscle to weaken, making repair more difficult. Degenerative tears in lower-demand patients are less time-sensitive and can often be trialled with physiotherapy first.
-
Traumatic rotator cuff tears resulting from an accident are generally eligible for ACC cover. Degenerative tears without a specific injury may not qualify for ACC and may instead be managed through private health insurance, self-funding, or referral to the public hospital system.
-
Most patients are in a sling for the first six weeks, with gradual return to normal activity over the following months. Full recovery, including return to sport or heavy manual work, typically takes six to twelve months.
-
Untreated tears, particularly full-thickness tears, can enlarge over time, and the associated muscle can weaken and develop fatty degeneration, which may make eventual repair less successful. Ongoing pain and functional limitation are also common if left untreated.