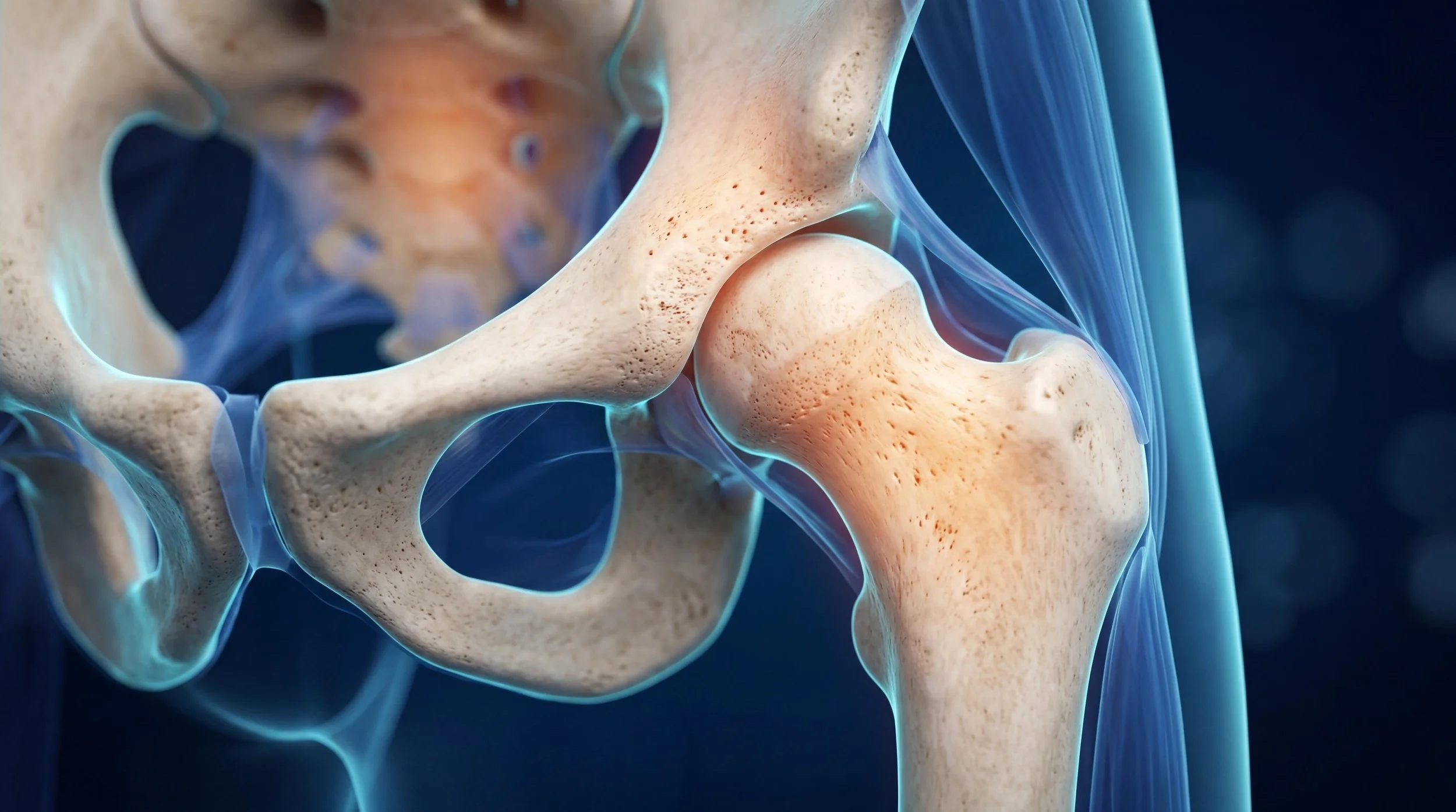
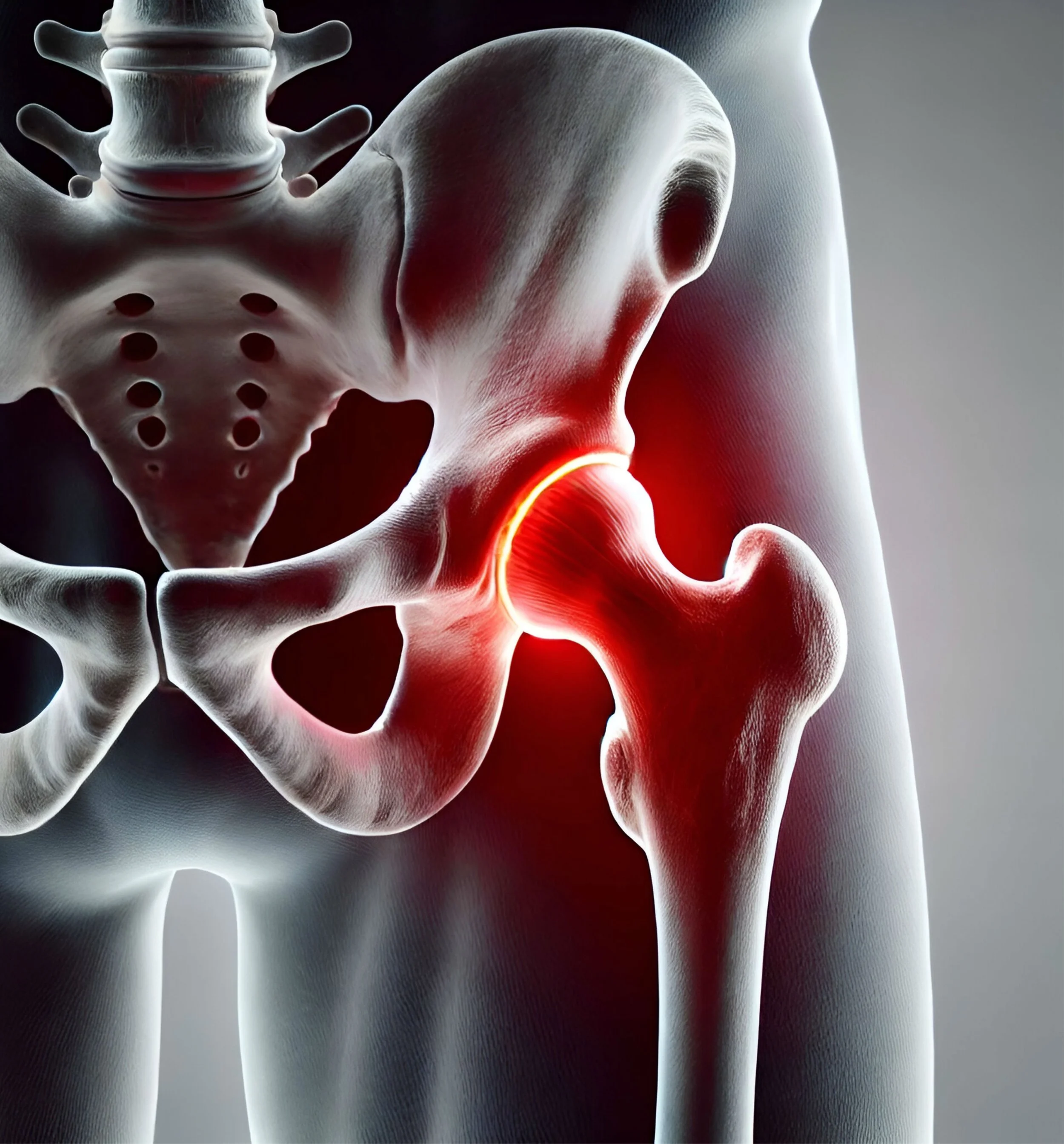
A hip labral tear is one of the most commonly misdiagnosed causes of deep groin pain in young adults - often labelled as a hip flexor problem or bursitis for a year or more before the correct diagnosis is reached. This guide covers what the labrum does, what causes it to tear, how it is diagnosed, and when treatment is appropriate.