
Deep groin pain that has not improved after months of physiotherapy is one of the most common presentations I see in my practice. In many of these patients, the underlying cause has been present for years - but labelled as a hip flexor problem, bursitis, or referred pain from the lumbar spine.
A hip labral tear is a structural injury to the cartilage ring that lines the rim of the hip socket. It does not heal on its own, and it does not respond to stretching. When it is associated with an underlying structural problem - which is usually the case - it will typically worsen over time unless the cause is addressed.
This guide covers what a hip labral tear is, how it is diagnosed, and when treatment is appropriate.
What is the hip labrum?
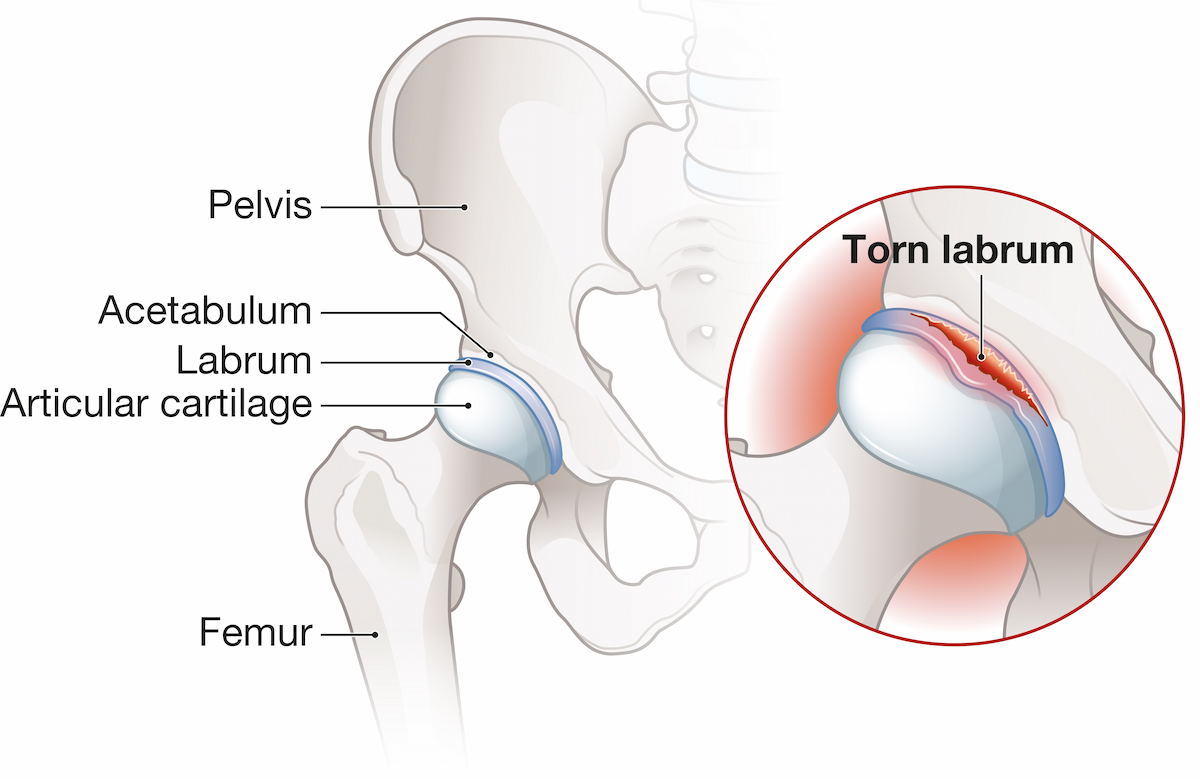
The labrum is a ring of fibrocartilage that lines the rim of the acetabulum - the cup-shaped socket of the hip joint. It serves several important functions: it deepens the socket and improves joint stability, it creates a seal that maintains the fluid pressure inside the joint, and it distributes load across the articular cartilage.
When the labrum is intact, it acts as a protective gasket for the hip joint. When it tears, that protection is lost. The fluid seal breaks, contact pressure increases on the cartilage, and - if the underlying cause is not addressed - cartilage damage may follow over time.
What causes a hip labral tear?
Most patients are unaware that hip labral tears are present in many active individuals without any symptoms - typically when there is no accompanying bony abnormality. Most symptomatic labral tears in young adults are caused by structural problems with the shape of the hip joint, rather than a single traumatic event. The two most common causes are femoroacetabular impingement (FAI) and hip dysplasia.
Femoroacetabular impingement (FAI)
FAI occurs when the ball (femoral head) and socket (acetabulum) have an abnormal shape that causes them to pinch against each other during movement. This pinching places repetitive stress on the labrum, eventually causing it to tear.
There are two types of FAI morphology. Cam impingement refers to an aspherical femoral head - the head-neck junction has too little offset, causing the extra bone to jam against the rim of the socket during hip flexion. Pincer impingement refers to overcoverage of the femoral head by the acetabular rim. Both types can occur together (mixed FAI), and both are associated with labral tears.
FAI is common in young active individuals - particularly those who played sport at a high level during adolescence - but it is not limited to athletes.
Hip dysplasia
Hip dysplasia refers to a shallow acetabulum - a socket that does not adequately cover the femoral head. When the socket is shallow, the labrum is recruited to compensate for the lack of bony coverage, placing it under sustained tensile load. Over time, this leads to labral tearing, often at the anterosuperior rim of the socket.
Dysplasia is more common in women than men and is frequently bilateral. It is often present from childhood and may not cause significant symptoms until early adulthood. It is important to identify dysplasia before treatment because labral repair alone, without addressing the underlying socket shape, has a high failure rate in dysplastic hips.
Acute trauma
A labral tear can also result from a single traumatic event - a fall, a sudden twisting injury, or a sporting collision. These traumatic tears may occur in hips with otherwise normal morphology, though in practice many patients who report a specific injury also have underlying structural vulnerability that was pre-existing.
Symptoms of a hip labral tear
The most common symptom is deep groin pain - typically described as pain inside the hip rather than on the outer hip or buttock. It is often described as aching or sharp, and may be difficult to localise precisely.
Other common symptoms include:
Pain that is worse with sitting for extended periods, particularly with the hip flexed past 90 degrees
Pain with driving, walking uphill, or rotating the hip
A clicking, catching, or locking sensation with certain movements
Pain that wakes you at night in some cases
A feeling of instability or giving way in the hip, particularly in dysplastic hips
It is common for symptoms to have been present for 12 months or longer before the correct diagnosis is reached. Labral tears are frequently misattributed to hip flexor tightness, bursitis, or referred pain from the lumbar spine - conditions that do not respond to the same treatment.
How is a hip labral tear diagnosed?
Diagnosis involves a clinical assessment combined with imaging. No single test is definitive on its own - the findings need to be considered together.
Clinical assessment
At your first consultation, I will ask about the location, character, and timing of your pain, what makes it better or worse, and your activity history. I will then examine the hip - assessing range of motion, strength, and performing specific provocation tests that reproduce your symptoms.
The FADIR test (flexion, adduction, internal rotation) is the most commonly used clinical test for labral pathology. A positive test does not confirm a labral tear, but in the right clinical context it provides important supporting evidence.
AP pelvis x-ray
An AP pelvis x-ray is the first and most important investigation. It allows assessment of the bony morphology of both hips - identifying FAI morphology (cam or pincer), dysplasia (a reduced lateral centre-edge angle), or other structural abnormalities that may be contributing to the problem.
An AP pelvis x-ray can be requested by your GP before referral and is a helpful starting point. Additional views - such as a frog-leg lateral or Dunn lateral - provide better assessment of cam morphology if FAI is suspected.
MRI arthrogram
If a labral tear is suspected after clinical assessment and x-ray, the gold standard investigation is an MRI or MRI arthrogram. An MRI arthrogram differs from a standard MRI: contrast is injected directly into the hip joint before the scan, which outlines the labrum and identifies tears, detachments, and associated chondral damage that a standard MRI may not reliably detect.
A standard MRI of the hip has slightly lower sensitivity for labral tears but avoids the need for a contrast injection and may be recommended in some cases. An MRI or MRI arthrogram is arranged through your specialist or orthopaedic surgeon after assessment and referral - it is not available through primary care in New Zealand.
Treatment options
Conservative management
Not all labral tears require surgery. In patients with small tears, no significant structural abnormality, and mild symptoms, a structured physiotherapy programme focused on hip stability and load management can provide meaningful improvement.
Conservative management typically involves a 10-12 week programme of targeted physiotherapy. If symptoms are improving, this can be continued. If there is no meaningful improvement after this period, or if symptoms are significantly limiting function, a surgical opinion is appropriate.
It is important to note that physiotherapy addresses muscle function and load distribution - it does not repair a torn labrum or correct the underlying structural abnormality (FAI or dysplasia) that caused the tear. In hips with significant structural pathology, conservative management may reduce symptoms temporarily but is unlikely to provide a lasting solution.
When is surgery considered?
Surgery is considered when:
Symptoms are significant and limiting daily activities or sport
There has been no meaningful improvement after a genuine trial of conservative management (typically 10-12 weeks of structured physiotherapy)
Imaging confirms a labral tear and identifies a structural cause (FAI, dysplasia, or both)
Joint space is preserved on x-ray - indicating that cartilage loss has not yet occurred
The timing of surgery matters. A labral tear repaired when the cartilage is still intact has significantly better outcomes than one treated after cartilage damage has occurred. This is why early assessment is worthwhile - not because surgery is always the answer, but because it keeps options open.
Hip arthroscopy for labral tears
Arthroscopic labral repair is a keyhole procedure performed under general anaesthetic, typically as an overnight case.
What the procedure involves
Two or three small incisions are made around the hip - each around a centimetre in length. A camera (arthroscope) is inserted into the joint, allowing me to directly assess the labrum, the articular cartilage, and the bony morphology of the hip.
The labrum is repaired using small suture anchors, which are inserted into the acetabular rim and used to reattach the torn labrum to the bone. If FAI morphology is contributing to the problem, the cam lesion is reshaped (femoroplasty) and any pincer overcoverage is trimmed (rim resection) at the same time.
In hips with significant dysplasia, labral repair alone is not adequate. These cases require a periacetabular osteotomy (PAO) - a procedure that repositions the socket to restore normal coverage - sometimes in addition to labral repair. This is discussed and planned before surgery.
What to expect on the day
You will be admitted on the morning of surgery. The procedure typically takes 60-90 minutes. You will be in recovery for one to two hours and then transferred to your room on the ward for observation. You will usually be discharged the following morning. Crutches are provided before discharge and are used for the first two to four weeks to protect the repair.
Recovery
Recovery from hip arthroscopy follows a structured timeline, guided by the body's healing process and monitored through physiotherapy.
Weeks 1-4: Crutches to protect the labral repair. Physiotherapy begins in the second week, focusing on gentle range of motion and neuromuscular control.
Weeks 4-8: Gradual progression to full weight-bearing without crutches. Physiotherapy continues with strengthening.
Months 2-4: Progressive strengthening, return to low-impact activity. Return to desk work is usually possible within one to two weeks of surgery.
Months 3-6: Return to sport and physically demanding work, depending on the extent of the repair and individual progress.
Physiotherapy is an essential component of recovery and not optional. The repair needs to be protected in the early weeks, then progressively loaded as healing occurs. Most patients work with a physiotherapist for three to six months following surgery.
When should I seek an orthopaedic opinion?
An orthopaedic opinion is appropriate if:
You have had deep groin or hip pain for more than three months that has not improved with physiotherapy
Your GP's x-ray has shown FAI morphology, dysplasia, or other structural findings
You have a clicking, catching, or locking sensation in the hip
Your symptoms are significantly limiting your daily activities, work, or sport
A normal x-ray does not rule out a labral tear. If the clinical picture fits and symptoms have not improved, a specialist assessment is still appropriate. The MRI or MRI arthrogram - the definitive investigation - is arranged through the specialist.
This article is for general educational purposes only and does not constitute medical advice. Please consult your doctor or seek a specialist referral for personal medical advice.